
This Friday, 24 February, SWZ Maritime's February issue will come out. The latest Mars Report can be read online now!
Mars (Marine Accident Reporting Scheme) Report is one of the regular sections of SWZ Maritime. We will publish all the reports we receive online, as they may prevent other accidents from happening. Mars Reports cover all kinds of maritime incidents such as (near) collisions and groundings, accidents with tools, falling objects injuring crew, accidents with rescue boats and so on.
Wet Nickel Ore Cargo Problems: Mars 201701
As edited from UK P&I Club Alert Bulletin 1113 – 10/16
Recently, the port of Surigao Philippines has experienced abundant rain. Mariners should be aware that unsafe wet nickel ore cargo is nonetheless being presented for loading at this port.
A number of ships that have recently loaded this cargo at Surigao have experienced problems. Extra vigilance is necessary should your vessel call at this port to load nickel ore cargo.
Lessons Learned
- Although crew can use ‘can’ tests to validate suspicions that the moisture content of the ore may be above the certified TML, the ore should also undergo an oven drying test in a laboratory.
- The Intercargo guide for transporting nickel ore, published in 2012, states: ‘Where there is doubt concerning any cargo declaration information, or suspicion that the cargo has been misrepresented, independent cargo testing to determine the Flow Moisture Point (FMP), Transportable Moisture Limit (TML) and actual moisture content of the cargo to be loaded should be carried out.’
- Cargo that appears wet and/or splatters when loaded may raise suspicions that the moisture content of the ore is above the certified transportable moisture limit.
More information is available in The Nautical Institute’s Knowledge Library.
Conflicting Mental Models: Mars 201702
As edited from official MAIB report 28-2015
A container vessel was leaving port in darkness under the con of a pilot. The third officer and the master were also on the bridge and a helmsman was steering by hand. On leaving the container ship, the pilot was scheduled to embark on an inbound tanker near the entrance of the buoyed port channel.
The tanker was approaching the entrance to the port channel and preparing to pick up the pilot. The master, the OOW and a helmsman steering in hand mode were on the bridge. The tanker was about one nautical mile (1nm) from No 1 buoy, making 126° COG at about 2kt. At about this time the port control authority was in an unrelated communication with a tug and had instructed the tug to ‘cross 1nm astern of the tanker’. The tanker’s master heard part of this radio exchange and assumed that port control was talking to the outbound container ship in relation to his ship.
The master of the tanker assessed that to pass astern of his vessel, the container ship would alter course to port on clearing the channel.
As the outbound container vessel was approaching No 3 buoy, the pilot and the master discussed the pilot’s disembarkation. The tanker was visible from the container vessel’s bridge in addition to showing on the radar displays, but it was not acquired as an ARPA target. Just before disembarking the container ship, the pilot advised the master to reduce speed to 10kt and to maintain 314° COG. By eye, the container vessel’s master estimated that the tanker would pass down his ship’s port side at a distance of 1.5 cables.
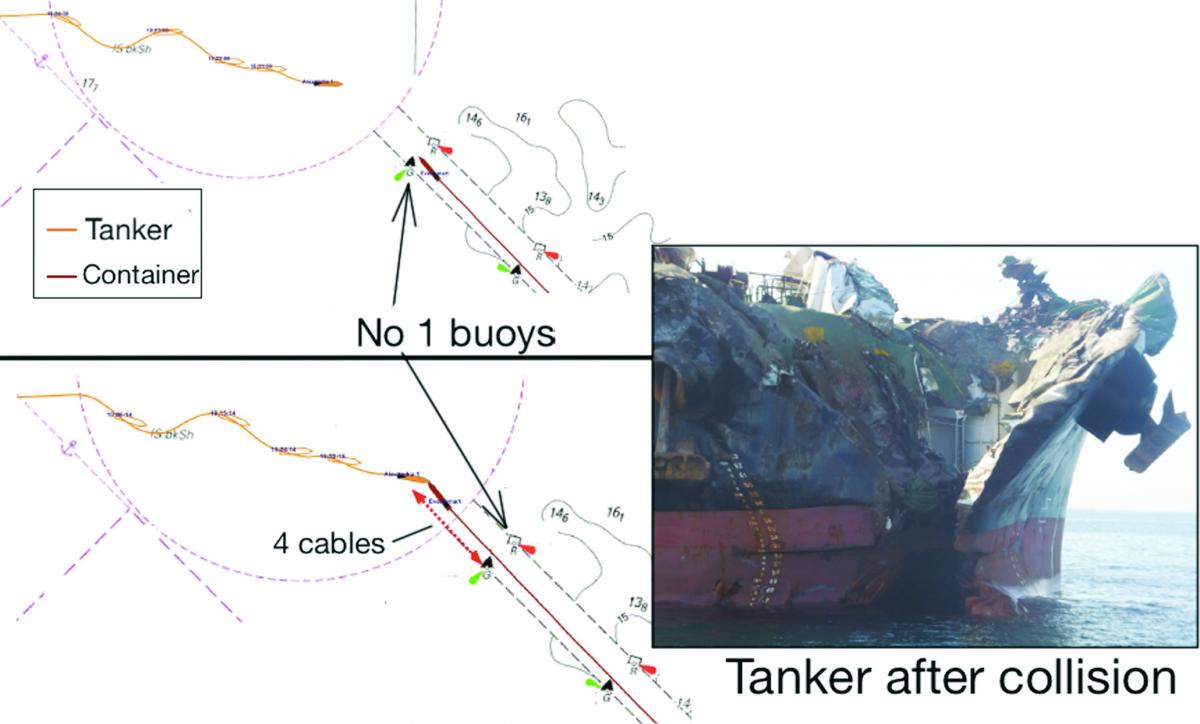
As the container vessel passed between the No. 2 buoys, the pilot launch with the pilot on board cleared the container vessel and headed towards the tanker. The container vessel’s master then increased the engine speed.
As the container vessel passed between the No. 1 buoys its speed was about 11kt. The tanker’s master saw the outbound container vessel pass between the No. 1 buoys and became concerned that the vessel had not altered to port as he had expected. He called VTS port control on the VHF radio to inquire. At this point, the pilot was still on the launch after having left the container ship. Shortly thereafter the two vessels, now both 4 cables from the entrance to the buoyed channel and near the centreline, collided bow to bow.
The official investigation found, among other things:
- The tanker master’s reliance on scanty VHF information and the failure of the container vessel’s master to keep a proper lookout and monitor the tanker’s movement were pivotal to this accident.
- A lack of an agreed plan and absence of effective communication, co-ordination and monitoring were significant factors, which contributed to the flaws in both masters’ situational awareness.
- On this occasion, the precautions of pilotage and port control, which should have been able to manage and de-conflict the vessels’ movements, were ineffective.
- The pilot’s failure to co-ordinate and communicate the passing arrangements for the two vessels was a significant omission; he was the assigned pilot for both ships. Although both masters were aware of the other vessel, the plan for the meeting of the vessels remained ambiguous.
Editor’s note: Although several factors contributed to this accident, the overarching paradigm remains that each master had a different mental model of the developing situation. Each made assumptions that, in the end, conflicted with the other’s.
Hydrodynamic Interactions While Berthing: Mars 201703
In daylight conditions and good visibility a passenger ship had turned on arrival in port and was making fast port side to berth. The vessel was in position with single springs fast fore and aft and was proceeding with head, stern and breast lines.
Another passenger vessel was passing between the berthing passenger vessel and a small bulker moored on the quay across the channel. It was estimated that the underway passenger vessel passed the berthing vessel at a lateral distance of approximately 30 metres. The maximum speed of the underway vessel while passing was 6.7 kt.
An officer on the berthing vessel was standing by to receive a shoreside gangway connection when he noticed the vessel starting to surge ahead and reported this to the bridge. The bosun on forward station simultaneously reported the forward spring coming under heavy strain.
Lessons Learned
The surge was most likely due to the hydrodynamic interaction caused by the underway passenger vessel passing at a very close lateral distance of 30 metres at a speed of more than 6kt.
The relatively narrow channel probably magnified interaction effects.
The surging of the moored vessel could have caused the spring line to part, which in turn could have caused serious personal injury or even death.
The officer posted on the bridge wing of the berthing vessel did not report the close approach of the underway passenger vessel sufficiently promptly. Had the officer done so, the bridge team might have been able to warn mooring station leaders to take extra caution and stand clear.
The entire bridge team must maintain situational awareness throughout the mooring process, and not relax and reduce alertness once vessel is in position with spring lines fast.
Hydrodynamic Interactions While Passing: Mars 201704
As edited from official TSB Canada report M05L0205
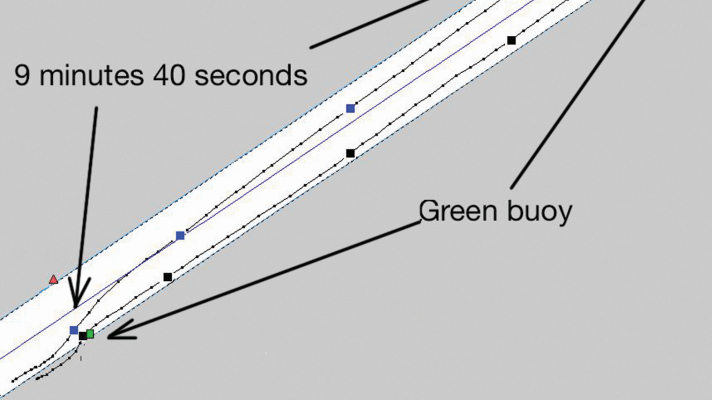
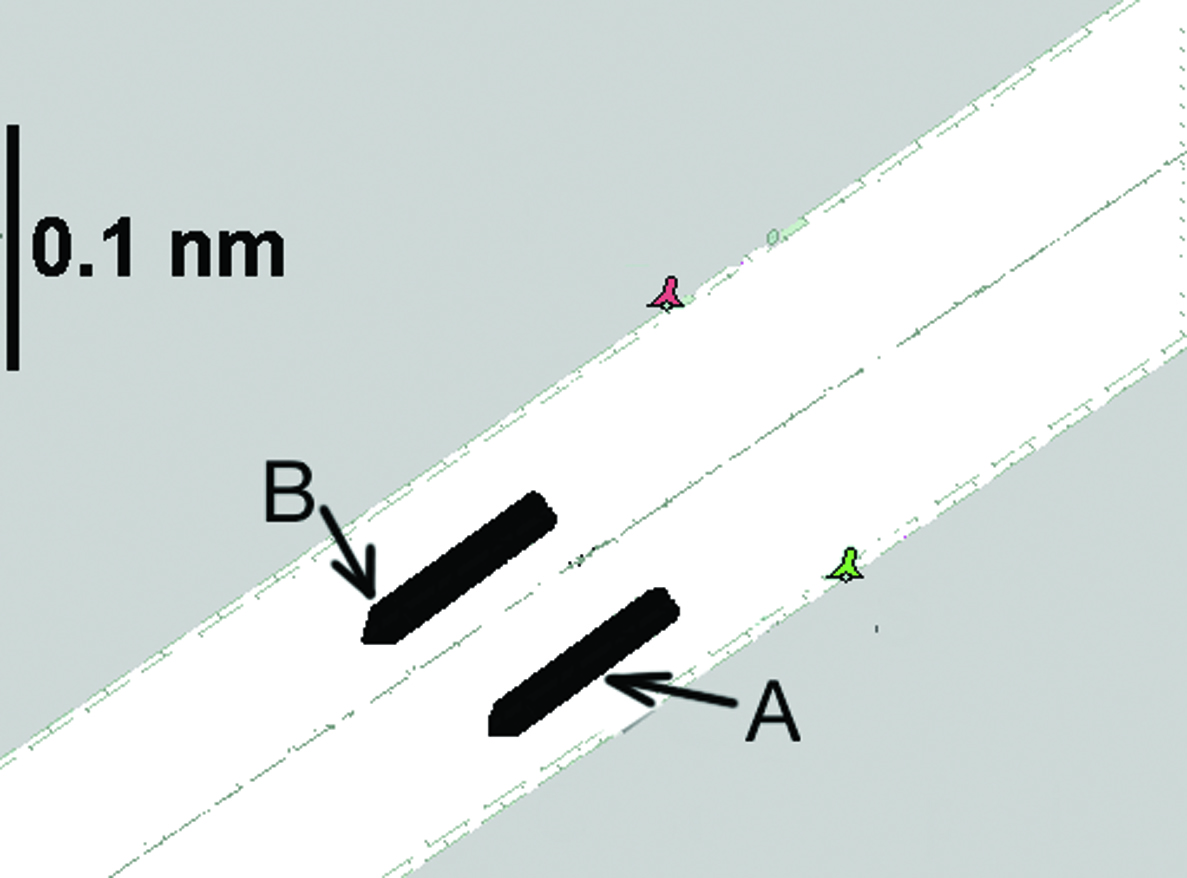
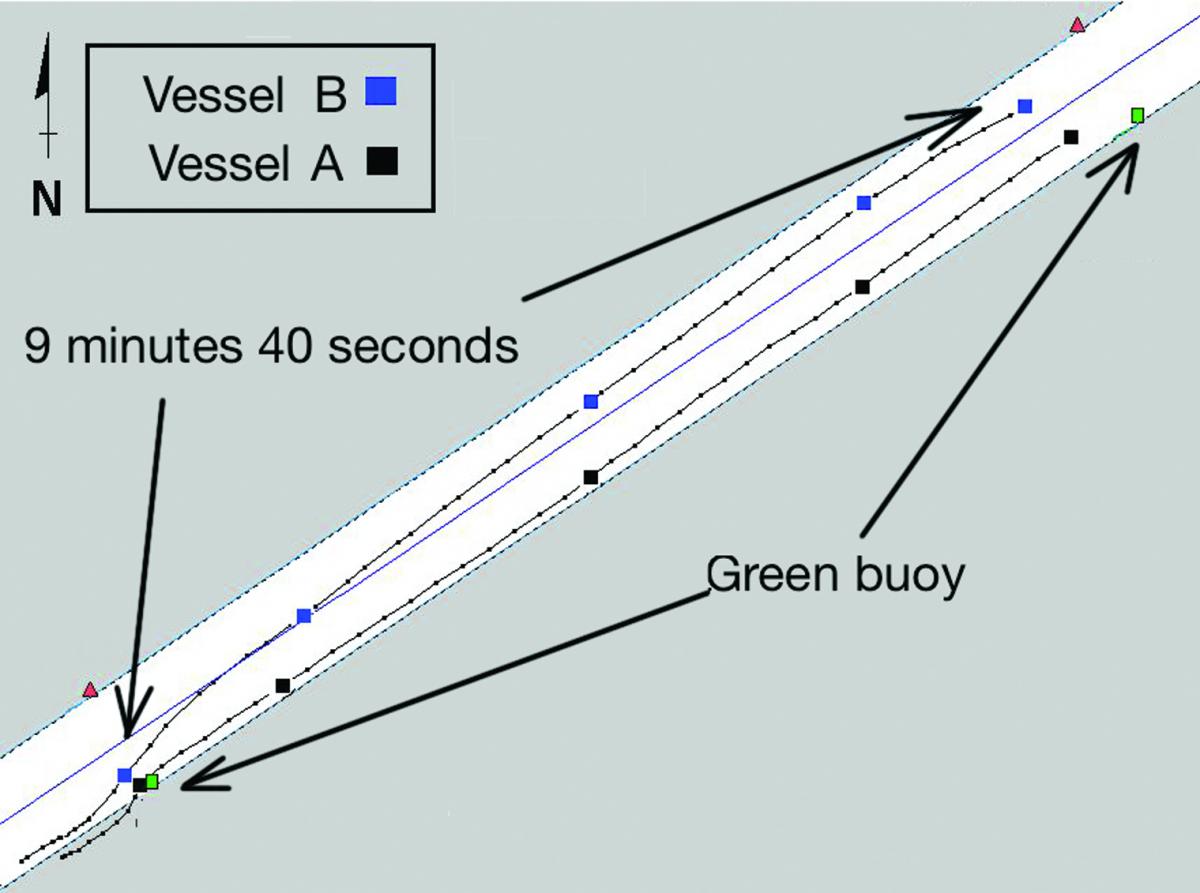
A container ship (A) had closed to approximately 8 cables astern of a loaded tanker (B) in a restricted waterway. The pilots of the two vessels had made overtaking arrangements; the tanker would move to the north side of the channel and reduce speed, and the container ship would also reduce speed, move to the south side of the channel, and overtake the tanker on its port side.
Ten minutes later, the helmsman on vessel A found it necessary to use a considerable amount of port helm (up to 23°) to maintain the desired heading of 235° Gyro (G). However, this information was not relayed to the pilot, nor did the pilot detect it from monitoring the rudder angle indicator. About one minute later, after passing a green channel buoy, the vessels were beginning to draw parallel to each other. They were now about 75 metres apart. Vessel B had reduced speed and was making 7.3 kt, and vessel A was proceeding at 10.7 kt.
A few minutes later, vessel B sheered suddenly to starboard. To regain control, the pilot ordered hard-a-port helm and half ahead followed by full ahead. Once the vessel steadied on a course of 236° G, the engine telegraph was reduced to dead slow ahead. Shortly afterward, there was no longer any apparent speed difference between the two vessels; both were proceeding at approximately 8 kt.
The pilot on vessel A then requested that vessel B further reduce speed so the vessel A could complete the overtaking manoeuvre. The pilot on vessel B agreed to the request, adding that he had just used ‘full ahead’ power to correct a sheer to starboard.
For the next five minutes, vessel A’s propeller pitch was modified incrementally on several occasions, resulting in an overall increase in speed from 8.2kt to 9kt. The changes were carried out by the OOW, who used his discretion to interpret the pilot’s orders, which were delivered in unquantified terms such as ‘faster’. As its speed increased, vessel A began to experience bank suction aft. The helmsman maintained the desired heading and prevented the bow from moving to starboard by applying more port helm. Again, this information was not communicated to any other members of the bridge team.
A few minutes later the pilot of vessel A asked the pilot on vessel B to further reduce speed. Pilot B replied that he was unable to comply without losing manoeuvrability. Moreover, vessel B’s speed had now increased from 7.3 to 8.2 kt despite the fact that there had been no change from the previous command of dead slow ahead. Despite full starboard helm at this point, vessel B continued to move towards vessel A.
For the next two minutes, the distance between the vessels continued to decrease. Even with vessel B’s engine telegraph set to stop, the tanker continued to accelerate to more than 8.5 kt. Aboard vessel A, the pilot requested greater speed and eventually full ahead.
With the vessels closing, pilot B asked for full ahead, in an attempt to pull away. Notwithstanding this action, the two vessels collided, making parallel body contact about 9 minutes 40 seconds after the overtaking manoeuvre had begun.
Some of the findings of the official report were:
- Neither pilot appreciated early enough the strength of the hydrodynamic forces at work, nor the need for early and decisive action to prevent the vessels from drawing together.
- Ineffective bridge resource management and poor communication between the vessels prevented both bridge teams from recognising the developing situation and taking timely action.
Lessons Learned
- When in the confines of a narrow channel, hydrodynamic forces between vessels are greater than when in open water due to the reduced flow capacity around the vessels and through the channel.
- When two ships pass or meet in the confines of a narrow channel, the squat experienced by each vessel increases by a considerable percentage.
- Hydrodynamic forces experienced by the vessels are proportional to the speed of the vessels through the water and inversely proportional to the distance between the vessels and the under-keel clearance of each vessel.
- The overtaking ship’s resistance increases once past the overtaken ship, and the latter’s resistance decreases. This can lead to a ‘trapping situation’ for the overtaking vessel.
- It is difficult to predict the onset and magnitude of hydrodynamic forces in the confines of a channel when manoeuvring large vessels.
- The hydrodynamic pressure zones around vessels can extend farther than the 100 metres commonly assumed.
Lively Dead Tow: Mars 201705
A barge was being brought into port as a dead tow by a tug under the con of a pilot. As the tug approached the fairway buoy at the port entrance, the towing gear of the tug began to part. The crew deployed one of the barge’s anchors and managed to prevent it from drifting into other vessels in the anchorage.
The tug crew recovered the damaged towing wire and changed to a second wire in order to hold the barge steady until a plan could be devised. The pilot requested tug assistance from the port but received no response. Pilot and master then decided to attempt to enter the breakwater, with the understanding that two harbour tugs would meet the barge at a point on passage, but this did not occur. The two tugs remained inside the breakwater as the tug and barge continued on passage in heavy wind and swells.
As this manoeuvre was unfolding the second towing wire parted. By this time two small harbour tugs were close at hand, though not made fast. Both tugs attempted to hold the barge in position but it ended up sideways in the main channel nonetheless, only just missing rocks as it swung through 90° in the main channel.
Lessons Learned
- Tug and towing gear should be appropriate for the job. In this case the tug and gear in question was rated at 68-tonnes bollard pull while the recommended bollard pull for the barge in question was 100t.
- Only one pilot was assigned for this complicated and delicate job.
- Best practice in many ports would be to assign two.
Battery Explodes: Mars 201706
As edited from Marine Safety Forum – Safety Flash 15-20
The electro-technical officer (ETO) was repairing an instant reaction electronic welder’s mask. The tablet-style lithium ion battery needed replacing, and because of the compact nature of the equipment it was considered that this could only be done by soldering connections on to the new battery.
The first connection was made successfully. While soldering the second connection, the battery overheated and popped, spraying the battery contents into the ETO’s eyes.
First aid was immediately administered by applying copious amounts of water to both eyes for 10-15 minutes using the emergency eye station sachets.
The master called for medical advice and was advised by an eye specialist to apply cortisone steroid drops three times daily and analgesic drops as necessary. The doctor did not feel medevac was necessary, but advised the master to monitor and call back if necessary.
After the first dose the victim’s eye condition improved rapidly, with a significant reduction in redness and irritation within 15 minutes. Fortunately for this crew member, the excellent emergency medical crew response on board meant that no permanent damage was sustained.
Lessons Learned
- Eye protection is essential when carrying out activities that have a risk of eye injury.
- Rapid and correct first aid response and treatment can make the difference between fast recovery and permanent injury.
- A risk assessment should always be carried out for unusual or uncommon jobs.
Acknowledgement
Through the kind intermediary of The Nautical Institute we gratefully acknowledge sponsorship provided by:
American Bureau of Shipping, AR Brink & Associates, Britannia P&I Club, Cargill, Class NK, DNV, Gard, IHS Fairplay Safety at Sea International, International Institute of Marine Surveying, Lairdside Maritime Centre, London Offshore Consultants, MOL Tankship Management (Europe) Ltd, Noble Denton, North of England P&I Club, Sail Training International, Shipowners Club, The Marine Society and Sea Cadets, The Swedish Club, UK Hydrographic Office, West of England P&I Club
Submit a Mars Report
More reports are needed to keep the scheme interesting and informative. All reports are read only by the Mars coordinator and are treated in the strictest confidence. To submit a report, please use the Mars report form and send it to mars@nautinst.org.


Lessons learned: also the
Lessons learned: also the battery room should be good accessible for battery service etc.